
The effect of using air rather than oxygen.
One of the advantages of a simulator is that it allows one to perform manouevres which are clearly unethical in the clinical situation. In this case, I've explored the outcome of ventilating the artificial lung with air (rather than oxygen) and then turning the ECMO system off altogether.
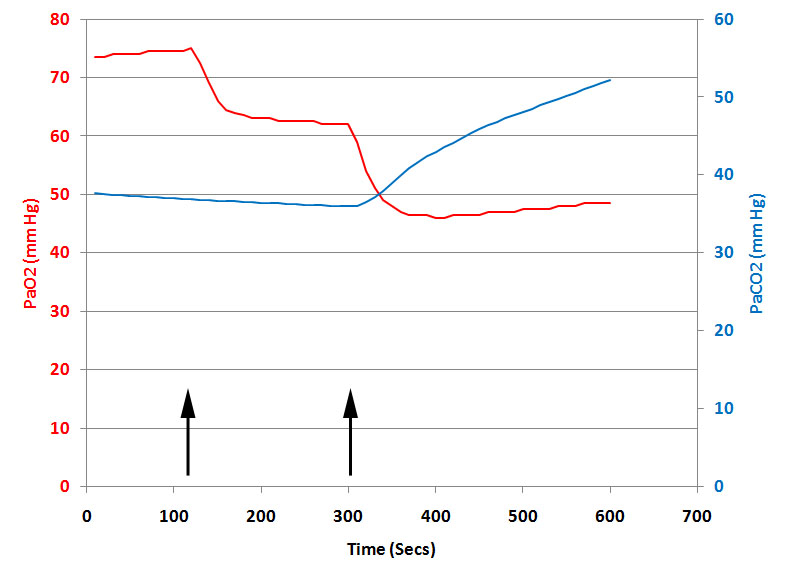
The data shown above are from a simulated patient with severe respiratory failure and an oxygen consumption of ~200 ml/min on stable VV ECMO. The patient has been completely paralysed with pancuronium and is ventilated on 100% oxygen with a tidal volume of 500 mls at 10 breaths per minute. Initially, the VV ECMO system has been set at a blood flow rate of 5.0 lpm, a ‘Sweep Gas’ flow rate of 4.0 lpm and an FiO2 of 1.0. The patient's native cardiac output is about 5 lpm.
At the first arrow, the FiO2 is abruptly reduced to 0.21 and at the second arrow the ECMO system is turned off completely.
When the switch is made to air ventilation, some oxygen transfer is still possible, but, because the pressure gradient driving oxygen across the membrane has been markedly reduced, the efficiency of transfer is significantly impaired. As a result, PaO2 falls quite markedly. In contrast, carbon dioxide transfer is completely unimpaired and PaCO2 does not change at all.
Turning the system off altogether causes a complete failure of both oxygen and carbon dioxide transfer.