Some of the manoeuvres undertaken in this tutorial generate extreme circuit pressures and are only intended to demonstrate the performance characteristics of the system. They should not be employed under clinical conditions.
In this simulation, we’ll continue to explore the characteristics of a Veno-Venous Extra-Corporeal Membrane Oxygenation (VV ECMO) system.
The learning objectives of the session are to investigate:
| • | The impact of return cannula size on ECMO system performance. |
We will be simulating the use of a system in a patient with essentially normal cardiovascular function, but with severe respiratory failure. The patient is a 24 year-old man, weighing 75 kgs, who has been transferred to your Intensive Care Unit for Veno-Venous ECMO.He had been admitted to the Intensive Care Unit of a large regional hospital 3 days before transfer to your institution. At that time, he presented a four day history of increasing respiratory distress, fever and a productive cough. The patient had been sedated, intubated and ventilated shortly after admission to the regional ICU. Blood and sputum cultures grew a methicillin-sensitive staphylococcus aureus. Despite treatment with appropriate antibiotics, the use of prone ventilation, permissive hypercarbia and inhaled nitric oxide, he continued to deteriorate. Following discussions with the clinicians at the regional hospital, he has been transferred to your institution for initiation of veno-venous ECMO. On arrival in your ICU the patient is being given assisted ventilation (via an ‘Ambu’ © bag) on 100% oxygen.
Blood gas analysis is reported as:
PaO2 |
44 mm Hg |
PaCO2 |
41 mm Hg |
pH |
7.34 |
BXS |
-3.5 |
Temp |
37.4 |
SaO2 |
73% |
The patient has an Acute Lung Injury Score (‘Murray Score’) of 3.5 but has no other significant co-morbidities. He has a Haemoglobin of ~ 12 gm/dL and you estimate his ‘shunt fraction’ (Qs/Qt) to be about 65%. The results of some ancillary investigations (Echo, CXR and ECG) are also available.
We’ll assume that you have already worked your way through VV ECMO tutorials (1) and (2), so we’ll quite quickly set up our monitoring:
| • | Click the <Display> button in the <Patient Monitor> window. |
| • | Check <ECG>, <Direct Arterial Pressure>, <Central Venous Pressure> and <SaO2> and |
| • | Click the <Display> button again to close this window and display the physiological signals. |
Ventilate the patient:
| • | Click the <Devices><Ventilator> menu item in the <Inspector> window. |
| • | Click the power switch at the top right-hand side of the device. |
| • | Set the tidal volume(Vt) to 500 mls, the rate to 10 bpm, the FiO2 to 100% and the PEEP to 5 cms H2O. |
Paralyse the patient:
| • | Click <Bolus Drug><Pancuronium (2mg/ml)>in the <Therapeutic Interface> window. |
| • | Drag the green slider until it says ~ 8 mgs and click the <Give> button. |
And perform a baseline blood gas analysis:
| • | Click <Investigations><Arterial Blood Gas Analysis>in the <Inspector> window. |
You elect to cannulate the patient percutaneously via the right and left internal jugular and right femoral veins using the Seldinger technique and ultrasonic guidance.
Imagine now that you have:
| • | Placed the Seldinger wires, |
| • | Given the patient 7500 units of heparin (Select <Heparin> from the <Therapeutic Interface> <Bolus Drug> page and <Give> 7500 units) and |
| • | Positioned the cannulae under ultrasonic control. |
You are using the same ECMO system that is similar to that described in VV ECMO Tutorials (1) and (2) – except that we are using two drainage cannulae. Active venous drainage from the inferior vena cava (IVC) is via a 24F femoral cannula, drainage of the SVC is via a right internal jugular cannula and ‘arterialised’ return to the right atrium via a 21F left internal jugular cannula (Figure 1.).
Figure 1.
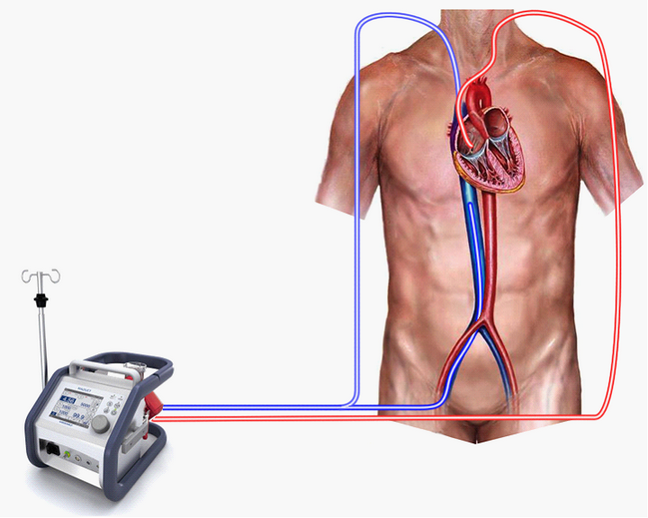
In this exercise, we’re only interested in the effect of changing the size of the return cannula, so we’ll make sure that the venous drainage is absolutely optimal. To do this:
| • | Switch to the ECMO system (Devices><ECMO System>). |
| • | Click <Adjust Cannula>. |
| • | Click <Dual Cannulation>. |
Advance the SVC drainage cannula:
| • | Slide the top left-hand slider down to <2> and |
Advance the IVC drainage cannula:
| • | Slide the bottom left-hand slider up to <8>. |
| • | Switch back to the ECMO system (Devices><ECMO System>). |
| • | Turn on the <Main Power>. |
| • | Set a gas flow of <6> lpm. |
| • | Fully open the arterial clamp. |
| • | Increase the blood flow to <4.0> lpm. |
Note the pre-membrane pressure (~130 mm Hg), and the rpm (~2375).
We’re now going to reduce the return cannula size from 21F to 15F. To do this:
| • | Click <Adjust Cannula>. |
| • | Click <Cannula>. |
| • | Select <15F>. |
| • | Click <Save>. |
| • | Switch back to the ECMO system (Devices><ECMO System>). |
Note that the blood flow has now fallen from ~ 4.0 lpm to ~ 2.9 lpm and the pre-membrane pressure has risen to (~150 mm Hg). To return the flow to 4.0 lpm you will need to increase the rpm to ~3100 (and the pre-membrane pressure will rise to about 250 mm Hg as a result). Thus, we can see that the resistance of the 15F cannula is much higher than that of the 21F cannula, and the ECMO pump has to work much harder to achieve a flow rate of 4.0 lpm.
Now let’s examine the effect of increasing return cannula size. To do this:
| • | Click <Adjust Cannula>. |
| • | Click <Cannula>. |
| • | Select <24F>. |
| • | Click <Save>. |
| • | Switch back to the ECMO system (Devices><ECMO System>). |
Note that the blood flow has now increased to ~ 4.4 lpm and the pre-membrane pressure has fallen to (~140 mm Hg). Return the flow to 4.0 lpm by decreasing the rpm to ~2500 and note that the pre-membrane pressure falls further to 115 mm Hg.
Figure 2.
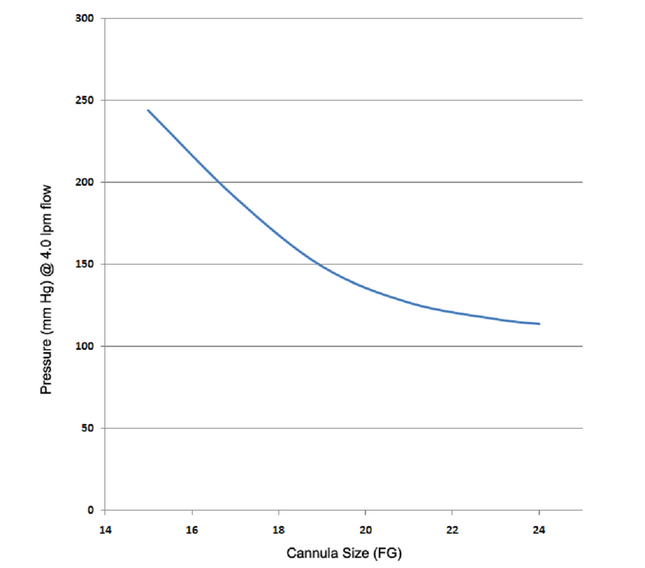
The pre-membrane pressure measurements for the complete range of cannulae at a flow rate of 4.0 lpm are summarized in Figure 2. Note how the pre-membrane pressure increases quite markedly once the return cannula size is reduced below 21F. Although there are no absolute rules for determining the maximum pressure which can be accepted within the ECMO circuit, it is believed that, ‘ceteris paribus’, higher pre-membrane pressures are more harmful than lower pressures.
There are several reasons for this belief.
| 1. | The use of small cannulae is inevitably associated with higher circuit velocities at any given flow rate. These higher velocities are associated with higher shear stresses on both red cells and platelets. Shear stress on red cells is a potential cause of haemolysis, and shear stress on platelets a potential cause of platelet activation. |
| 2. | Smaller cannulae require higher rpm to achieve a given flow rate. These higher rpm require more energy delivery by the pump which in turn tends to increase the operating temperature of the system and the ‘thermal stress’ on the blood. |
| 3. | Smaller cannulae are associated with a greater amount of exit turbulence and a more marked ‘sand-blasting’ effect. |
| 4. | Higher circuit pressures pose a greater risk of circuit disruption. |
Thus, the take home message (in adults) is to use a 21F return cannula if possible.
This concludes the exercise.