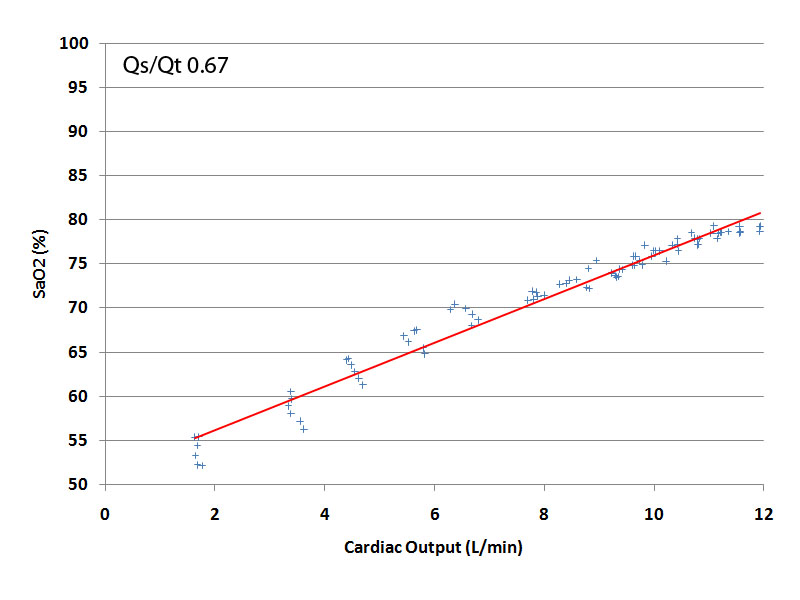
The effect of cardiac output on SaO2 when Qs/Qt is constant.
Almost all patients in severe, acute respiratory failure have a large right-to-left shunt ('Qs/Qt' or 'Shunt Fraction') and, in the case of patients requiring ECMO, this fraction is typically more than 60%.
Before we consider the effect of a reduction in cardiac output (CO) on arterial saturation in those on VV ECMO and the effect of an increase in cardiac output on arterial saturation in those on VV ECMO, we need to understand what happens to SaO2 in such patients (in the absence of ECMO), when cardiac output changes.
In the figure below, I've recorded what happens to SaO2 in a 75 kg patient with a large right-to-left shunt (67%) when the patient's cardiac output increases from under 2 L/min to more than 12 L/min.
As can be seen, the arterial saturation rises from less than 55% at the lowest cardiac output to about 80% at the highest. This increase in arterial saturation occurs primarily because the increased CO leads to an increase in the saturation of the mixed venous blood. As a result, when the mixed venous blood passes through the right-to-left shunt, it contains relatively more oxygen and is therefore less effective at causing hypoxia.